Does Raw Camel Milk Cure Autism?
In late 2025, the FDA quietly removed a consumer advisory page from its website titled “Be Aware of Potentially Dangerous Products and Therapies that Claim to Treat Autism.” The page had been live since at least 2019 and warned parents against a range of unproven autism “treatments,” including chelation therapy, hyperbaric oxygen chambers, chlorine dioxide (industrial bleach), and — lumped in with the rest — raw camel milk.
The Department of Health and Human Services told ProPublica the page was retired “during a routine clean up of dated content.” Many autism researchers and advocacy organizations weren’t buying that explanation, noting that the warnings themselves were still accurate and still necessary. The removal drew significant media attention — including from the BMJ — in part because it coincided with HHS Secretary Robert F. Kennedy Jr.’s broader effort to reshape federal health messaging around autism, including reconstituting a federal autism advisory committee with proponents of several of those same unproven treatments.
The controversy renewed public interest in the claims around raw camel milk specifically. This article examines what the science actually shows — without reflexive dismissal and without credulous hype.
Autism Has No Cure
Autism spectrum disorder (ASD) is a genetic configuration that is often exacerbated by the environment, not a disease to be eradicated or “cured.” The characteristics of autism — differences in social communication, sensory processing, and patterns of behavior — are considered by many autistic people and advocates to be core aspects of their character, not pathology to be reversed.
Many families with autistic children, particularly those with profound autism (~26.7% of autism cases), are actively searching for approaches that might address specific co-occurring challenges: anxiety, digestive issues, sleep disruption, behavioral regulation, and chronic inflammation. That search is good and important, their sometimes excessive open-mindedness is understandable. The difficulty is that the marketplace of “autism cures” has historically been filled with exploitative and outright dumb non-solutions — from chemical chelation to bleach protocols that have killed children.
Raw camel milk does not belong in that category. It is also not a cure. Let’s have a look at the existing research.
The Biological Case for Camel Milk in ASD Research
Camel milk has a nutritional profile that differs from cow milk in ways that are directly relevant to the biological features associated with autism. It is lower in lactose, contains no beta-casein A1 (the protein variant linked in some research to inflammatory gut responses), and is richer in immunoglobulins, lactoferrin, and antimicrobial peptides. Its antioxidant and anti-inflammatory properties are well-documented in the literature.
The relevance to ASD lies in a substantial body of evidence showing that many autistic children exhibit elevated oxidative stress and chronic neuroinflammation — higher levels of inflammatory biomarkers and lower levels of antioxidants such as glutathione. If camel milk modulates those pathways, there is a biologically plausible rationale for why it might affect certain symptoms.
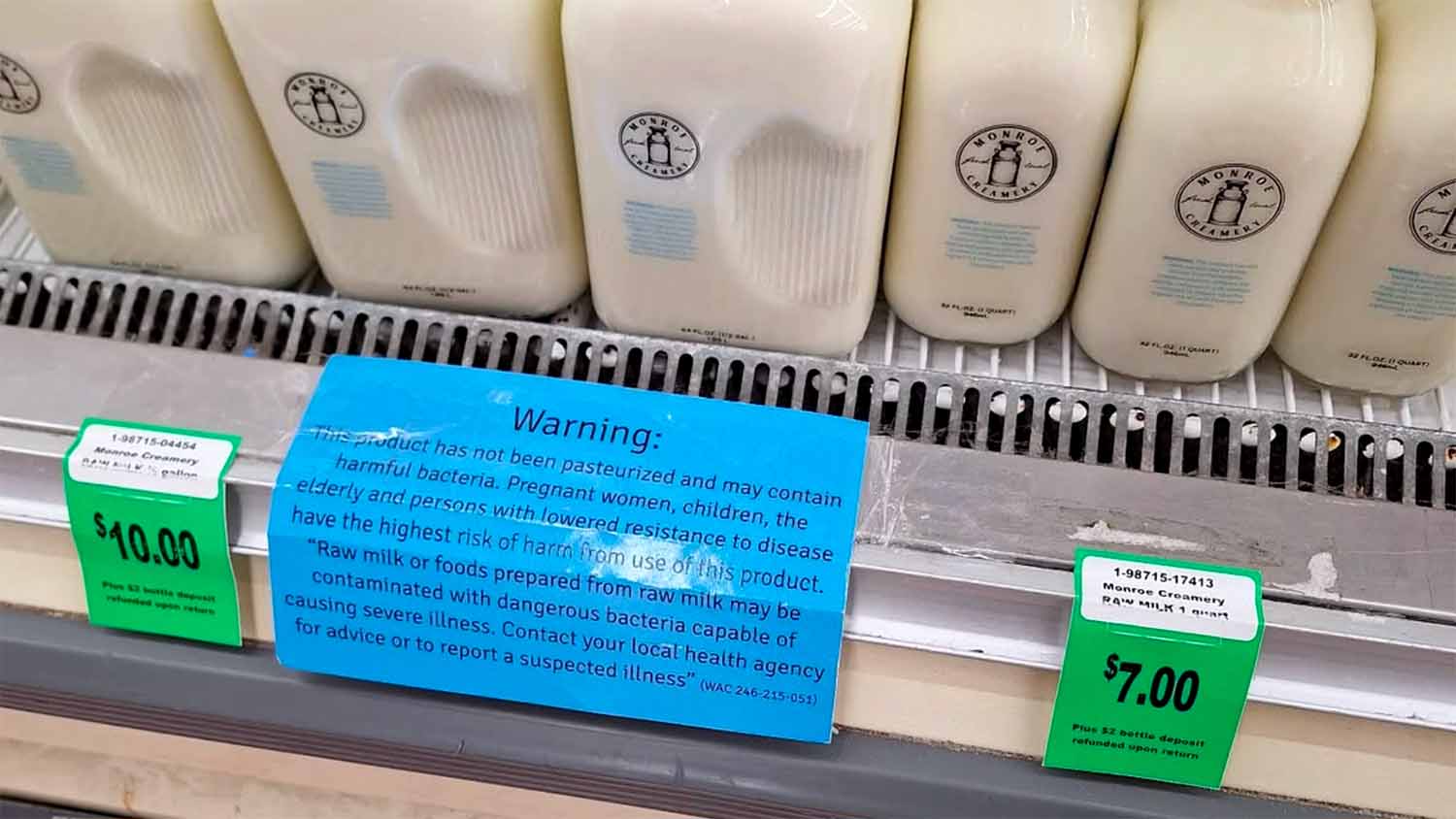
Raw camel milk, specifically, is thought to preserve more of these bioactive compounds than pasteurized or boiled versions, as heat degrades certain immunoglobulins and enzymes. This is part of the broader argument for raw milk’s nutritional superiority — and it explains why the raw form has been the focus of the most clinically significant individual trials.
What the Clinical Research Shows
The research is mixed. The evidence base is preliminary but not negligible, and the honest assessment sits somewhere between dismissal and endorsement.
Trials Showing Positive Effects
Several small randomized controlled trials (RCTs) conducted primarily in the Middle East — where camel milk has a long history of traditional medicinal use — have found statistically significant improvements in autism rating scale scores among children who consumed raw camel milk compared to those who received cow’s milk as a placebo.
One double-blind study published in Pediatric Research found that raw camel milk, but not boiled camel milk, produced a significant improvement in Childhood Autism Rating Scale (CARS) scores, alongside a significant decrease in serum levels of thymus and activation-regulated chemokine (TARC), an inflammatory marker. In plain terms: children who drank raw camel milk showed measurable improvements in autism severity scores and reduced inflammation compared to the control group.
Other trials have documented that both raw and boiled camel milk increased plasma levels of glutathione, superoxide dismutase, and myeloperoxidase in autistic children — all markers involved in the body’s antioxidant defense systems. A 2022 study found significant reductions in TNF-alpha, a key pro-inflammatory cytokine, in children consuming camel milk compared to placebo.
A separate meta-analysis covering studies through 2022 found that both raw and boiled camel milk were associated with lower CARS scores than placebo, with raw camel milk showing a mean difference of 2.77 on the scale — a clinically meaningful shift.
The 2024 Meta-Analysis: Pumping the Brakes
The most comprehensive and rigorous analysis to date was published in late 2024 in the Open Veterinary Journal. Researchers searched multiple major databases and identified 5 RCTs involving 299 children that met inclusion criteria for quality analysis.
The verdict: the mean difference in CARS scores between camel milk and control groups was not statistically significant overall (p = 0.23). The subgroup analysis for raw camel milk specifically also fell short of significance (p = 0.18). However — and this is important — the qualitative synthesis did find that raw camel milk intake was associated with improvements in various social behaviors and increases in antioxidant and anti-inflammatory biomarkers.
The authors concluded that camel milk “shows promise” but that larger, more rigorous trials are needed before conclusions can be drawn. A 2015 double-blind RCT from King Saud University that assessed 65 autistic children using CARS, the Social Responsiveness Scale (SRS), and the Autism Treatment Evaluation Checklist similarly found behavioral improvements and reached the same conclusion: promising, but more research needed.
Interpreting the Evidence
The overall picture is consistent with early-stage research: individual trials finding real effects, a pooled analysis losing significance due to small sample sizes and heterogeneous study designs, and biological data pointing in a plausible direction. This is what “promising but unproven” looks like in the scientific literature. It is categorically different from dangerous quackery, and it is categorically different from established therapy.
Why It Appeared on the FDA’s Warning List
Raw camel milk was placed on that page alongside chlorine dioxide (an industrial bleach that some parents were persuaded to administer to autistic children) and chelation therapy (which has killed children when misapplied). The range of risk across those products is vast, and the grouping was imprecise.
The FDA’s stated concern about raw camel milk was not that the substance itself is inherently dangerous. It was a food safety concern: that parents seeking autism treatments might source raw camel milk from unregulated suppliers without adequate pathogen controls. Raw milk of any species carries a risk of contamination if not properly handled and tested.
That is a legitimate concern about sourcing and supply chain — not a pharmacological warning. Properly sourced raw camel milk from a farm with rigorous testing protocols is a food product with a real, if preliminary, evidence base. The FDA’s original framing did not make that distinction, placing it in the same category as substances that have caused direct harm to children.
Milk from other species
Cow’s milk serves as the placebo in most of the camel milk RCTs, and the data from those trials is telling: when the 2022 meta-analysis compared responsiveness across groups, cow milk consumers showed a mean CARS improvement of only -1.02 — compared to 1.99 for boiled camel milk and 2.77 for raw camel milk. So cow’s milk has been directly compared to camel milk in controlled trials and has performed substantially worse on autism severity scores.
Goat’s milk has attracted genuine research interest for similar reasons to camel milk — it contains predominantly A2 beta-casein rather than A1, higher levels of omega-3 fatty acids (EPA and DHA), and prebiotic oligosaccharides that resemble human breast milk. A 2023 study published in Metabolites from King Saud University — some of the same researchers behind the camel milk trials — investigated goat’s milk versus cow’s milk in a valproic acid-induced rat model of autism, hypothesizing that lower casein levels and higher EPA/DHA content might help reduce autistic features. The study found the goat’s milk intervention produced improvements in neurotransmitter and oxidative stress markers compared to cow’s milk, though the researchers noted more in-depth studies and clinical trials are needed. Crucially, this was an animal study — there are no published RCTs of goat’s milk in autistic children comparable to the camel milk trials.
Donkey milk sits in a similar position to goat’s milk: there is anecdotal and community interest, particularly among families dealing with what may be PANDAS/PANS (autoimmune-related neurological conditions that can present with autism-like behaviors), but no clinical trials in humans specifically for ASD. The donkey research that does exist focuses primarily on animal-assisted therapy (i.e., interacting with donkeys), not consuming their milk.
Why camel milk stands out: The research advantage camel milk holds over goat and donkey milk isn’t necessarily that it’s categorically superior — it’s that it has actually been studied in human RCTs. Researchers note that camel milk’s small immunoglobulins are similar to those found in human breast milk, which is one of the distinguishing factors cited for its immunomodulatory potential. Camel milk also notably lacks beta-lactoglobulin entirely, an allergen present in cow’s, goat’s, and sheep’s milk that causes reactions in sensitive individuals, which may make it more tolerable for children with dairy sensitivities.
So in short: goat’s milk has a plausible biological rationale and some animal-model data; donkey milk has community-level interest but essentially no ASD-specific research; and cow’s milk has been directly tested as a control and consistently underperformed camel milk in the trials that exist. Camel milk’s lead in the literature is partly a function of where the research has been conducted (Saudi Arabia, where camels are culturally significant and researchers have prioritized this question) rather than a definitive proof that it is biochemically superior to all other non-bovine milks.
Summary
Raw camel milk is not a cure for autism. There is no cure for autism. Any product or practitioner using that language should be treated with skepticism. The clinical evidence for raw camel milk is preliminary: individual trials have found measurable improvements in autism severity scores and inflammatory biomarkers, but the most rigorous pooled analysis to date did not find statistically significant effects when those trials were combined. The biological mechanisms are plausible and actively studied. The risks associated with raw camel milk are primarily those of any raw dairy product — a function of sourcing quality rather than the substance itself.
The FDA’s decision to list it alongside industrial bleach and chelation therapy reflected an imprecision in categorization that the agency never adequately explained. The subsequent removal of the entire warning page — whatever its political context — leaves families with less public guidance on the full spectrum of autism-related products, from the genuinely dangerous to the merely unproven. Those are different things, and families deserve information that treats them as such.
Sources
- Kandeel M, et al. (2024). Meta-analysis of the efficacy of camel milk consumption for improving autism symptoms in children in randomized clinical trials. Open Veterinary Journal, 14(9), 2441–2452.
- Al-Ayadhi L, Elamin NE. (2013). Camel milk as a potential therapy as an antioxidant in autism spectrum disorder. Evidence-Based Complementary and Alternative Medicine.
- Al-Ayadhi L, et al. (2022). Comparative study on the ameliorating effects of camel milk as a dairy product on inflammatory response in autism spectrum disorders. Neurochemical Journal, 16(1), 99–108.
- Bashir S, Al-Ayadhi L. (2014). Effect of camel milk on thymus and activation-regulated chemokine in autistic children: double-blind study. Pediatric Research, 75(4), 559–563.
- Al-Ayadhi L, et al. (2015). Behavioral Benefits of Camel Milk in Subjects with Autism Spectrum Disorder. Journal of the College of Physicians and Surgeons Pakistan, 25(11), 819–823.
- Kandeel M, El-Deeb W. (2022). The Application of Natural Camel Milk Products to Treat Autism-Spectrum Disorders: Risk Assessment and Meta-Analysis of Randomized Clinical Trials. PMC.
- O’Matz, M. (February 18, 2026). Chlorine Dioxide, Raw Camel Milk: The FDA No Longer Warns Against These and Other Ineffective Autism Treatments. ProPublica.
- Adams, J. (January 2026). FDA removes web page warning of dangers of unproved autism treatments. BMJ.
- FDA Consumer Update: Be Aware of Potentially Dangerous Products and Therapies that Claim to Treat Autism(archived, 2019).