Certified Milk: America’s First Raw Milk Production Standard
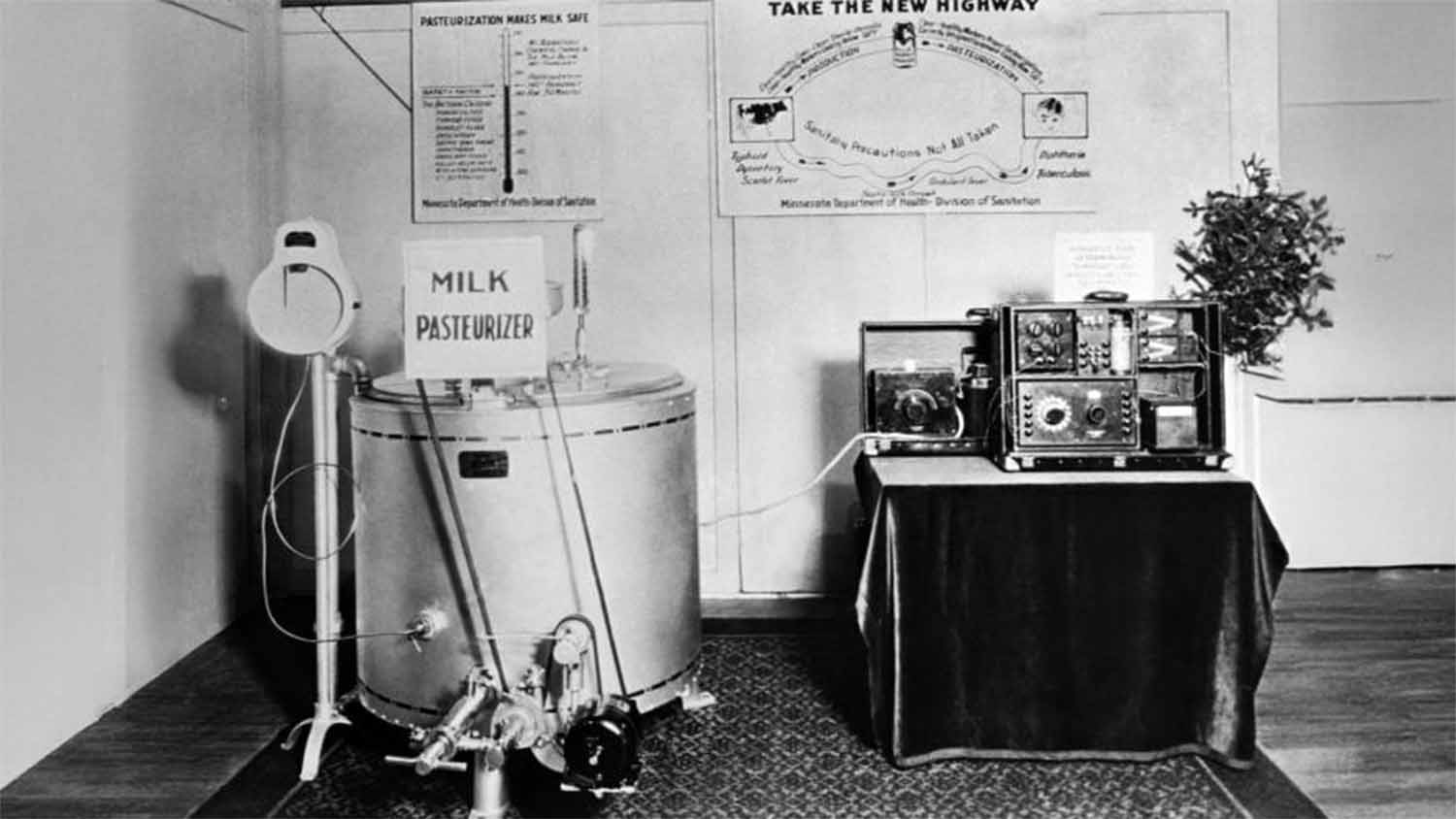
At the 1929 Minnesota State Fair, the Minnesota Board of Health set up a working pasteurizer on the fairgrounds, complete with a thermocouple display and wall-mounted messaging explaining how heating milk made it safe to drink. The photograph survives in the CDC’s public health image library. It captures something that tends to get lost in pasteurization history: the technology did not sell itself. It had to be demonstrated, explained, and endorsed by government agencies at venues designed to reach ordinary people. That officials felt compelled to do this in 1929 is evidence that pasteurization was not yet a settled conclusion.
Pasteurization mandates were not competing with ignorance or farmer resistance to regulation. Certified milk was their opposition, a formal, physician-led quality standard for raw milk that had been operating for decades.
Henry Coit and the Essex County Origin Story
Henry Leber Coit was a Newark pediatrician who had been pressing the Medical Society of New Jersey since 1889 to investigate an urgent and fundamental question: how do you secure clean milk for patients and the public? His concern was personal. For two years he had sought a reliably clean milk source for his infant son, whose mother had been unable to breastfeed successfully. The search culminated in a small suburban dairyman who kept four cows and delivered milk daily to the Coit household, a man who, as Coit later wrote, was “an honest and industrious man, but without knowledge of hygiene.” The man became an unwitting danger.
The commodity raw milk of that era was drawn from cows kept in overcrowded urban dairies, often fed distillery byproduct mash, handled without sanitation protocols, and transported without refrigeration. Infant mortality rates exceeded 200 per 1,000 births, and infantile diarrheal disease was a major contributor. No mechanism existed to distinguish the milk of a careful small farmer from the output of a filthy urban dairy operation. Both arrived at the door unlabeled and indistinguishable.
Coit’s answer was contractual and physician-led. In April 1893, he enlisted colleagues to form the Essex County Medical Milk Commission, which entered into contract with a New Jersey dairyman named Stephen Francisco of Caldwell. Francisco agreed to produce milk under conditions the Commission specified: clean udders, clean hands, sterile containers, healthy cows, tested workers, suitable housing, careful feed. The resulting product would carry a copyrighted and trademarked label: “Certified Milk.” The name belonged to no single producer; it belonged to the standard.
Coit described the plan as providing “a commission of medical men who, with the support of physicians generally, should, by voluntary supervision, paid expert inspection, and final certification, endeavor to influence a supply of milk produced under regulations imposed by themselves.” Quality assurance, third-party verified, financed through inspection fees, sold at a price premium to a market willing to pay for the differentiation.
What Certification Actually Required
The requirements that emerged from the Essex County model were substantive. Certified milk farms operated under veterinary inspection schedules that included tuberculin testing of the herd, a meaningful threshold in an era when bovine tuberculosis was a genuine transmission risk. Workers underwent periodic medical examinations. Milking equipment was cleaned and sterilized between uses. Milk was bottled at the farm and cooled immediately, not held in open transport containers for hours.
The bacteriological standard was the most quantifiable dimension. Certified milk was required to contain no more than 10,000 bacteria per cubic centimeter at delivery to the consumer. That threshold was achievable only through rigorous on-farm hygiene, and it was dramatically lower than ordinary commercial milk of the period, which could carry counts in the millions per milliliter. For context, the federal Pasteurized Milk Ordinance today sets the Grade A raw milk limit at 100,000 colony-forming units per milliliter, ten times higher than what certified milk producers were expected to achieve more than a century ago.
The AAMMC’s 1909 published manual organized its standing committees around four pillars: medical examination of employees, chemical standards, bacteriological standards, and veterinary inspection with attention to tuberculosis. The physicians who contributed to those reports included figures prominent in American public health at the time, among them W.H. Park and M.J. Rosenau, lending institutional weight to what remained a voluntary, privately administered program.
How the Standard Spread Nationally
The Essex County model spread quickly. New York adopted it in 1896, Philadelphia in 1897. By 1909, 58 local Medical Milk Commissions were operating across the United States, each formulating its own requirements while converging on the same essential framework. In 1907, most federated into the American Association of Medical Milk Commissions (AAMMC), which harmonized standards nationally and published a uniform methods manual.
The AAMMC held no regulatory authority. Its power was reputational and market-based: the “Certified Milk” label could appear only on milk produced in compliance with the published Methods and Standards, supervised by a locally recognized commission, and tested against defined bacteriological limits. States and municipalities eventually incorporated this into their own regulatory language. A voluntary private standard had acquired quasi-regulatory status through adoption by public authorities.
The standard also scaled beyond small boutique operations. The Walker-Gordon Laboratory Company, established in Plainsboro, New Jersey in 1897, grew into what the Smithsonian Institution Archives describes as the world’s largest certified dairy farm by 1930, operating under the AAMMC framework and producing certified milk for markets in New York and Philadelphia.
Certified milk was a premium product prescribed by physicians for infants and the ill, sold at roughly two to four times the cost of ordinary commercial raw milk. That premium reflected real costs: expert inspection visits, veterinary examinations, laboratory testing, specialized bottling and cooling equipment, and the small herd sizes that rigorous sanitary conditions required. The system was a niche quality market, not a mass-market solution, and was designed with that limitation understood.
The Competing Logic: Nathan Straus and the Economic Case for Pasteurization
Running parallel to Coit’s work was a campaign led by Nathan Straus, co-owner of Macy’s and a New York philanthropist who concluded that pasteurization, not inspection, was the only scalable answer to urban milk contamination. Starting in 1893, Straus opened a network of milk depots across lower Manhattan, distributing pasteurized milk to poor families at nominal cost. Statistics showing drops in infant mortality in those neighborhoods became his evidence for heat treatment at urban scale. (The story of how pasteurization came to be industrialized in America is bound up with these early figures and their competing philosophies.)
The operative word was scalable. For Straus and the officials who backed him, pasteurization was a matter of economics and practicality. Most acknowledged that certified milk was safe, but at two to four times the commodity price it was out of reach for the urban populations most exposed to contaminated milk. Rather than patrol farms with their own inspectors, cities chose to require pasteurization and let companies absorb the cost of the equipment. This push toward centralization drove the creation of ever-larger middlemen that could aggregate fluid milk from many farms and process it in one place.
Between 1915 and 1924, the U.S. Public Health Service reported an increase in pasteurization of milk sold in cities over 10,000 from 6 to 45.7 percent. By 1947, that figure had reached 90 percent. The regulatory choice made in those decades did not merely resolve a public health question. It shaped the structure of the American dairy industry for the rest of the century.
The “Dirty Milk” Argument and the Public Campaign
The Minnesota State Fair pasteurizer exhibit was a document of deliberate public persuasion. The 1920s were precisely the period when state and local health agencies were consolidating around pasteurization as policy, and when advocates recognized that legal mandates worked better with public cooperation than against public suspicion.
The sharpest objection from certification advocates was that pasteurization enabled producers to sell dirty milk, heating the pathogens out rather than maintaining clean production from the start. If producers know heat treatment will sterilize whatever they deliver, the economic incentive for on-farm sanitary discipline is reduced. The certified milk model had worked precisely by tying economic reward to sanitary performance. Farms that met standards earned the premium; farms that could not did not receive certification. Pasteurization, critics argued, severed that feedback loop.
The argument appeared not only among raw milk advocates but in mainstream public health literature. A 1923 British public health publication mordantly suggested the lowest milk grade might reasonably be labeled “A.O.D.S.,” standing for “Any Other Dirty Stuff.” In 1936, British dairy producers formally protested a government order that would have permitted the term “Certified” on pasteurized milk labels, arguing it borrowed the movement’s hard-won reputation to market a heated product.
The lobbying and institutional campaigns that drove compulsory pasteurization laws into American cities were not purely scientific processes. They involved public education campaigns, commercial interests, and political relationships that accelerated the policy beyond what the science alone demanded. The history of the swill milk scandal makes clear that the “dirty milk” concern was grounded in actual conditions. What the certified milk movement argued was that those conditions demanded sanitary reform at the source, not thermal correction after the fact.
How Certified Milk Declined
The two approaches coexisted for roughly four decades. Commercial dairy interests who stood to benefit from centralized processing saw in pasteurization mandates an opportunity to restructure the market, and the regulatory outcome reflected that complexity.
The Great Depression removed the economic foundation on which certified milk depended. Retail milk prices collapsed in the early 1930s, dropping more than a third in some markets. A product priced at two to four times the commodity rate required customers with discretionary income. That customer base shrank dramatically after 1929. The inspection overhead that made certification credible did not disappear; the market willing to pay for it did.
Federal milk marketing orders introduced through the Agricultural Adjustment Act of 1933 and revised in 1937, part of the New Deal’s broader restructuring of agricultural markets during the Depression, standardized the regulatory framework around pasteurization as the baseline safety expectation. Certified raw milk remained a legal category in some jurisdictions but ceased to function as a commercially significant national movement. By mid-century it had become a footnote, a decline accelerated by postwar media campaigns including a 1945 Coronet magazine article that helped drive the first statewide raw milk ban in Michigan three years later.
The Standard’s Longer Significance
The certified milk movement did not decline because its standards were wrong. It declined because a premium quality program for a niche market could not survive a decade-long economic collapse, and because the regulatory framework constructed afterward was built around industrial processing rather than farm-level accountability.
What certified milk demonstrated was that a privately administered quality system, built on measurable bacteriological standards, third-party inspection, herd health documentation, farm-level bottling, and a consumer-facing certification mark, could function at scale. The AAMMC ran this model across 58 cities for roughly four decades. Organizations like RAWMI, the Raw Milk Institute, operate on a similar structure today, with individual farm risk management plans, regular standard plate count and coliform testing, and public result reporting, within a very different regulatory environment but toward the same end.
The AAMMC’s 10,000 CFU standard was met through inspection contracts, small accountable herds, and farm-level bottling, decades before refrigerated trucking or centralized testing labs existed. RAWMI-affiliated farms today meet or beat that same figure using updated tools but largely the same underlying discipline: clean animals, clean handling, and verified results before milk reaches a consumer. Coit’s commission set out in 1893 to make raw milk measurably safe at its source. A farm-level testing program today exists to answer the same question.